What is Rasha Disease? Causes, Symptoms and Treatments
Rasha disease is a neurodegenerative condition affecting dopaminergic neurons in the brain leading to associated motor symptoms. Neurodegeneration means a progressive irreversible loss of neurons. In Rasha disease, it is mostly the dopamine-producing neurons in the substantia nigra that are lost.
Rasha disease in Urdu
رعشہ کی بیماری دماغ میں ڈوپامینرجکنیورونز کو متاثر کرنے والی ایک نیوروڈیجینریٹو حالت ہے جس سے منسلک موٹر علامات پیدا ہوتی ہیں۔ نیوروڈیجنیشن کا مطلب نیورونز کا بتدریج ناقابل تلافی نقصان ھے۔رعشہ کی بیماری میں، زیادہ تر ڈوپامین پیدا کرنے والے نیوران جو سبسٹینشیا ناگرا میں موجود ہوتے ھیں ،ضائع ہو جاتے ہیں۔
Rasha disease in English
Rasha disease is the Urdu name of a disease more commonly known as Parkinson’s disease
Pathophysiology
For us to move signals are generated by the cerebral cortex that then pass through the motor pathways. This leads to the contraction of our muscles and ultimately movement. However, this process needs to be regulated which is primarily the job of basal ganglia. The substantia nigra is a part of the basal ganglia which are a group of nuclei in the brain. These are the striatum which includes the putamen and caudate nucleus. Amongst others, there is globus pallidus, subthalamic nucleus, and of course the substantia nigra.
Normally there are two main Pathways that control movement, the Direct and Indirect pathways. The direct pathway is an excitatory pathway that facilitates movement in which the motor cortex sends excitatory signals via Glutamate to the striatum. The striatum then sends inhibitory signals to the globus pallidus internal and substantia nigra pars reticulata via GABA. These two both release GABA which normally inhibits the Thalamus. So in this pathway, there is inhibition of the inhibition on thalamus giving an overall increased activity of the thalamus which promotes movement.
The indirect pathway is instead an inhibitory pathway whose purpose is to terminate movement. In this case, there is an inhibitory GABA signal from the striatum to the Globus pallidus external. The Globus pallidus external normally inhibits the subthalamic nucleus which normally stimulates the Globus pallidus internal. This means that the indirect pathway increases the inhibitory effect of the Globus pallidus internal on the thalamus. So there is less signal from the thalamus and so there is less movement.

How does Dopamine work?
In Rasha disease there is a gradual degeneration of neurons within the substantia nigra pars compacta. These neurons release dopamine to the striatum. In the striatum, there are direct pathway neurons that have D1 dopamine receptors and are excited by dopamine, and indirect pathway neurons that have dopamine D2 receptors and are inhibited by dopamine. Overall this means dopamine released from the substantia nigra pars compacta increases movement by stimulating the direct pathway and inhibiting the indirect pathway activity. So when these neurons are lost the opposite occurs. There is less stimulation of the direct pathway and less inhibition of the indirect pathway, meaning an overall reduction in movement
It is thought that the degeneration of these neurons is due to the accumulation of alpha-synuclein. This protein is involved in the regulation of the synaptic vesicles and the release of neurotransmitters. This is the same protein accumulation found in Lewy Body dementia. That is why the two diseases are believed to be closely related.
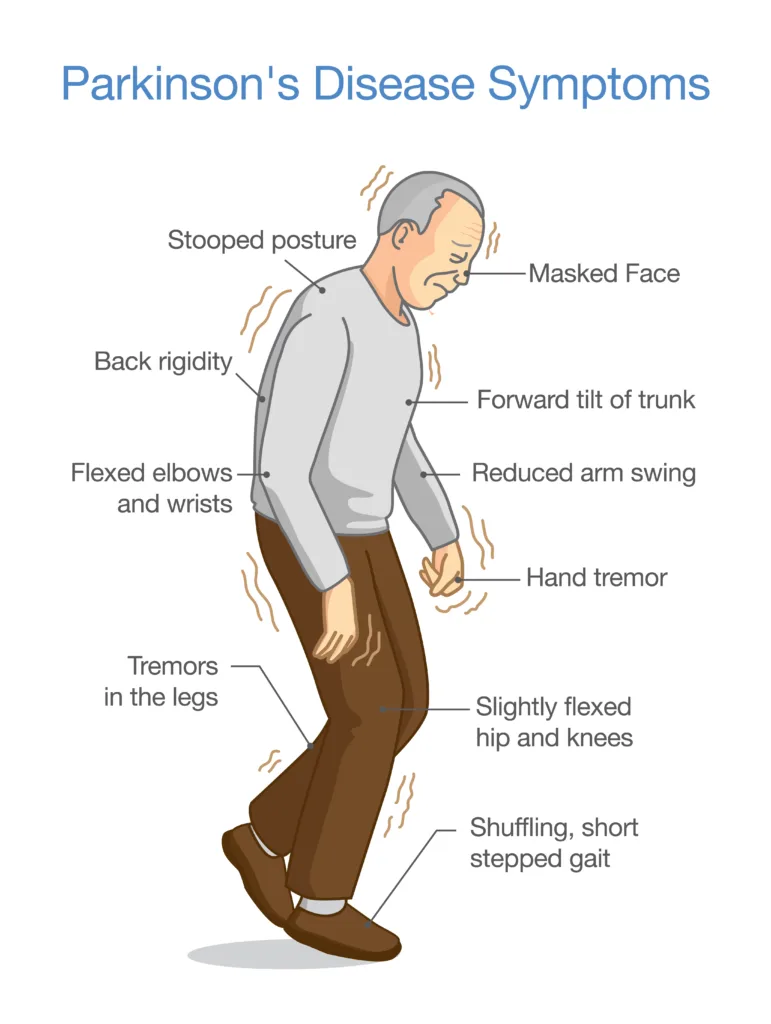
Rasha Disease Symptoms
Symptoms linked with Rasha disease occur when around 50 percent of the total neurons are lost. The symptoms that develop are unsurprisingly largely linked to movement. Bradykinesia which means slow movement is a core feature of Rasha/Parkinson’s disease. Rigidity is another core feature meaning stiffening of the muscles. The two types of rigidity in Rasha disease are cogwheel rigidity and lead pipe rigidity. Cogwheel rigidity means small start and stop movements like a gear. In lead pipe rigidity, there is an increased resistance throughout the range of motion.
A combination of rigidity and bradykinesia is what gives the mask-like face in Rasha’s disease known as hypomimia. Another feature is tremors in particular a pill-rolling tremor. Given its name because it affects the index finger and thumb making it resemble rolling a pill. Tremors in Rasha disease also tend to disappear during movement and reappear at rest known as resting tremors. Gait is often affected and patients will take several steps to turn, small steps with no heel strike or toe off often called a shuffling gait. Generally, Rasha disease patients are at an increased risk of falls.
Collectively these signs and symptoms are known as Parkinsonism and Rasha disease makes up around 80 percent of cases. However, there can be other causes such as drug-induced, multi-system atrophy, progressive supranuclear palsy, and normal pressure hydrocephalus. Other symptoms seen in Rasha disease can include autonomic disturbance like hypersalivation, constipation, and incontinence. Varying degrees of cognitive impairment can also be present.
Causes/Risk Factors of Rasha’s Disease
The reasons why neurons are lost in Rasha disease are not clear and most cases are idiopathic, meaning no specific cause is found. It is believed that there is a genetic link as first-degree relatives seem to have twice the risk than others. Between 10 and 15 percent of cases are believed to be familial with a mixture of both autosomal dominant and recessive inheritance patterns.
Environmental factors are also thought to increase the risk of Rasha disease. These include living in rural areas which may be due to exposure to Industrial or farming chemicals as well as infections including Encephalitis. Age seems to be the largest risk factor. The mean age of onset of Rasha disease is 60 however it is estimated that 5 to 15 percent of cases actually manifest before the age of 40. It is estimated that one percent of people over the age of 60 have Rasha disease. It is also slightly more common in males than it is in females.
Diagnosis of Rasha Disease
The diagnosis is mostly clinical as there is no specific laboratory or Imaging tests available. There is a new set of criteria called the Movement Disorder Society Parkinson’s disease criteria. These require parkinsonism meaning bradykinesia and one of resting tremor or rigidity. On top of that, there must be two supportive criteria, no absolute exclusion criteria, and no red flags. The supportive criteria examples are an improvement in symptoms with dopaminergic treatment or levodopa-induced dyskinesia. Exclusion criteria could be Parkinsonian features limited to the lower limbs for more than three years or treatment with dopamine receptor blockers coinciding with the symptoms.
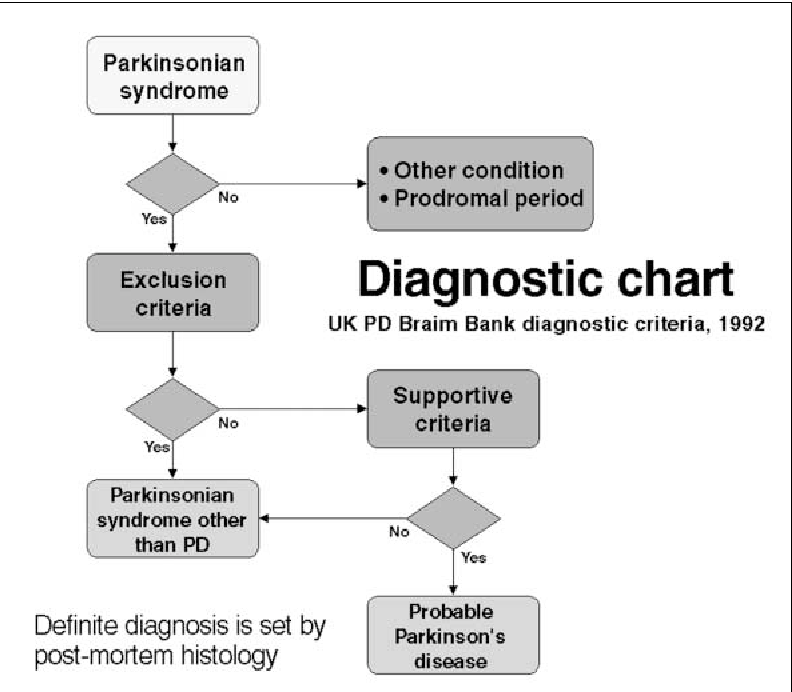
Red flags could be a rapid progression of gait impairment, symmetrical parkinsonism, or severe autonomic failure. A DaT scan or radioactive isotope is injected that binds dopaminergic neurons followed by a single photon emission computed tomography scan can be done to highlight areas of dopaminergic neuronal loss, but this is not widely available
Treatment of Rasha disease
Although Rasha disease does not have a cure, there are options to combat the symptoms. Medications are used to improve the quality of life although they do not generally slow down the progression. Increasing dopamine in the central nervous system is the goal, however, dopamine itself cannot be given as it does not cross the blood-brain barrier. Whereas levodopa, a precursor to dopamine can. The problem however is that levodopa is broken down peripherally by the enzyme Dopa decarboxylase and therefore an inhibitor like a Carbidopa is often given to increase the amount of levodopa reaching the brain.
Pramipexole and Ropinirole are dopamine agonists. Selegiline is a monoamine oxidase B inhibitor where monoamine oxidase B breaks down primarily dopamine and the Amantidine can be used as it increases dopamine synthesis and reduces its reuptake. Tolcapone and entacapone are catechol-o-methyl transferase Inhibitors which is also an enzyme that breaks down levodopa but these have been associated with liver toxicity.
On/Off phenomenon in Rasha disease

Initially, medication may treat the symptoms well. However, as time goes on there is less of an effect and the on/off phenomenon almost inevitably appears with the use of levodopa. Over time the window for controlled symptoms known as the on phase gets tighter while off is a state of rigidity and uncontrolled symptoms. The switch from on to off and vice versa can happen quickly like the change of a light switch.
Dyskinesia are involuntary movements that are a side effect that can occur when patients flip between on and off phases known as diphasic dyskinesia. It can also occur following levodopa medication, giving Peak dopamine levels known as Peak dose dyskinesia. In patients who no longer gain benefits from medication, deep brain stimulation could be an option. A pulse-generating device like a heart pacemaker is placed under the skin near the clavicle with electrodes connected to areas of the basal ganglia to improve function.
If you find this article useful please let us know in the comments. Also, check out our other articles about similar topics on our blog page.